A 100 TAVR anesthesia guardian, personal thinking about such surgery
Author:Anesthesia Medical Group Time:2022.09.03
1. What is TAVR surgery?
The so -called TAVR, translated into Chinese names: TAVR replacement (TAVR, Transcatheter Aortic Valve Replacement), and some people are translated into tavi surgery, and the content of the two is consistent. This surgery is an internal intravascular catheter technology that loads the artificial valve into the pipe system. The artificial valve is transmitted to the aortic valve position to release it through peripheral blood vessels or aperture.
2. What kind of patients are suitable for recommended TAVR?
TAVR's first surgery reported time in the world was in 2002 and introduced domestic domestic in 2012. At that time, there were only 4 centers that can independently complete surgery in China. In 2020, domestic single centers that can independently complete surgery exceeded 100 for the first time. At present, according to reports, there are more than 400 single centers that can independently complete surgery in China.
According to the ACC/AHA Guide (American Cardiology Society), for patients with high risk patients who cannot withstand surgical surgical treatment or surgery, they are recommended to prefer the aortic valve replacement of TAVR surgery. For example: elderly patients (patients who are recommended for foreign guidelines are more than 80 years of age); patients with a long history and poor mental function; there are many patients in patients, such as merging diabetes, lung function, renal insufficiency, digestive tract diseases, etc. Patients with complications; patients have previously undergone chest opening surgery. Patients need to be performed again for cardiac surgery this time. Tavr surgery can be preferred to replace the aorta.
3. What are the advantages of TAVR compared to the traditional open chest aorta replacement?
Compared with the traditional open -thoctoral circulation underneath the aortic valve replacement, the TAVR surgery is exempted from the traditional aortic valve replacement surgery requires the damage of the chest open. Patient's surgical trauma greatly reduces the risk of surgery. Patients will not be like a traditional thoracic operation after surgery. There are large surgical wounds from the upper nest of the sternum to the sword, and there will be no postoperative pain. Generally, there is a penetration point at the unilateral or bilateral groin. Compared with the traditional thoracic proofing of the thorax, the anesthesia time and surgery time are relatively shortened compared to the traditional opening of the thoracic procedure. Generally, the overall time of the patient is completed within 120-150 minutes. The patient feels good after surgery. Generally, after 24 hours of surgery, you can get out of bed. He will be hospitalized for 3 days after surgery.
4. What is the life of the TAVR valve?
At present, Tavr surgery, the valves used are biological valves. At present, the internationally recognized gold standard is the cow -hearted valve produced by Edward. According to the current report, the life of the biological valve is generally 10-15 years after surgery, and then the biological valve may occur in calcification damage. According to the clinical situation, the narrow or (and) is not fully closed. Aortic vector.

5. Patients need to undergo TAVR surgery. When the valve is selected, is it imported or domestic?
At present, my country has been approved by CFDA and can be used in clinical TAVR valve. All of them are Chinese independent intellectual property valve products. The results of clinical trials are not significantly different from similar foreign products. The aortic valve reflux TAVR valve is also applied abroad.
6. The anesthesia method and choice of TAVR surgery?
There are three methods for anesthesia in China at present TAVR surgery:
1) Trail intubation full hemp;
2) Non -insertion general anesthesia (bureau hemp+enhanced MAC);
3) Luan Ji Monitoring.
If patients need to undergo TAVR surgery, anesthesia doctors should fully evaluate the patient's past medical history, general conditions, current medical history and internal medicine complications, and choose the most suitable way of anesthesia for patients. Regardless of the choice of any of the three anesthesia methods, the single center experience of the anesthesiology center of Beijing Anzhen Hospital also needs to prepare for the patient's anesthesia alternatives according to the pneumatic intubation to prevent accidents during the operation.
7. Taking the tracheal intubation under the general anesthesia, complete the TAVR surgery as an example. After the patient enters the room, what do we need to do as anesthesia workers?
1) First of all, we should fully communicate with the patient to eliminate or reduce the patient's anxiety and fear, and obtain the trust and cooperation of the patient;
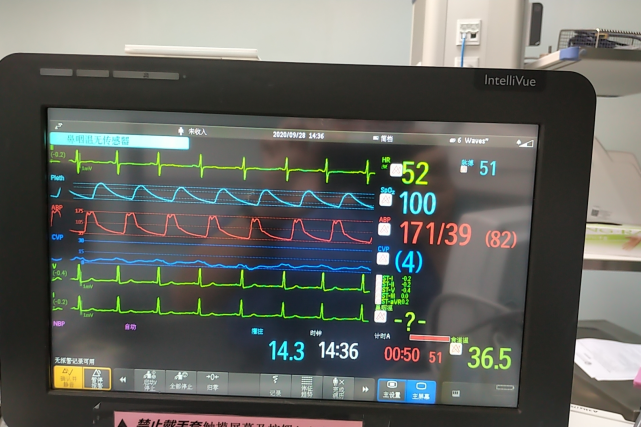
2) Give patients to monitor the five -guided links, blood oxygen monitoring, evaluate the patient's preoperative electrocardiogram status, and closely monitor various vital signs. The liquid support of the effective flow rate flow, and do a good job of the warmth and warmth of the patient at the same time;
3) Re -evaluation according to the condition, consider the establishment of the central vein pathway and the monitoring of the central vein pressure before considering the induction of anesthesia as appropriate;
4) The central vein pathway is established and the general hemp induction. After the bronchial intubation is completed, it is properly fixed, continuously monitoring the various vital signs of patients, and maintaining the depth of anesthesia and the stability of blood flow dynamics.
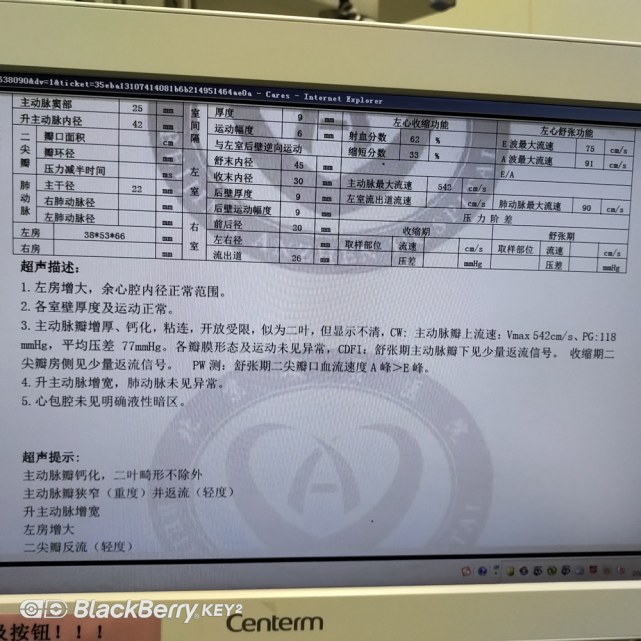
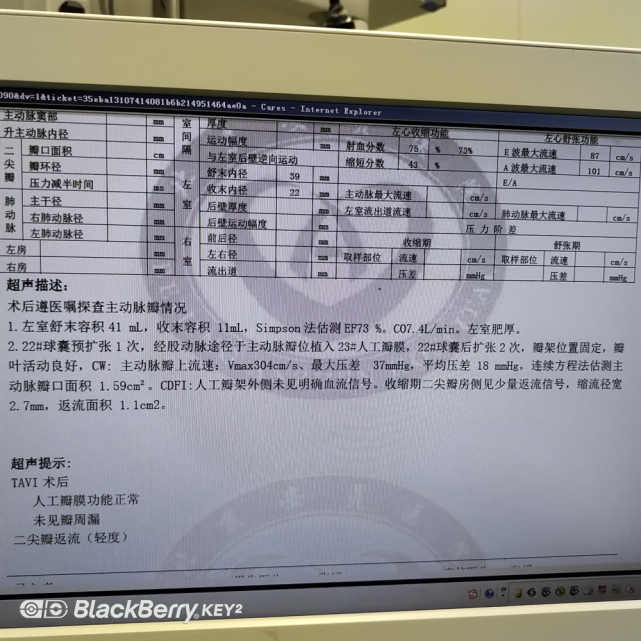
5) According to the patient's condition, conduct a gallery/chest ultrasonic diagram, and the last time before surgery performed ultrasound diagnosis and conditional assessment.
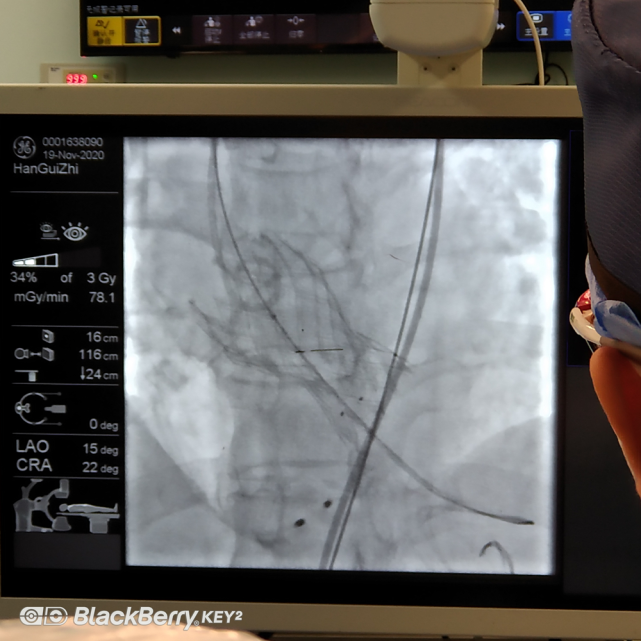
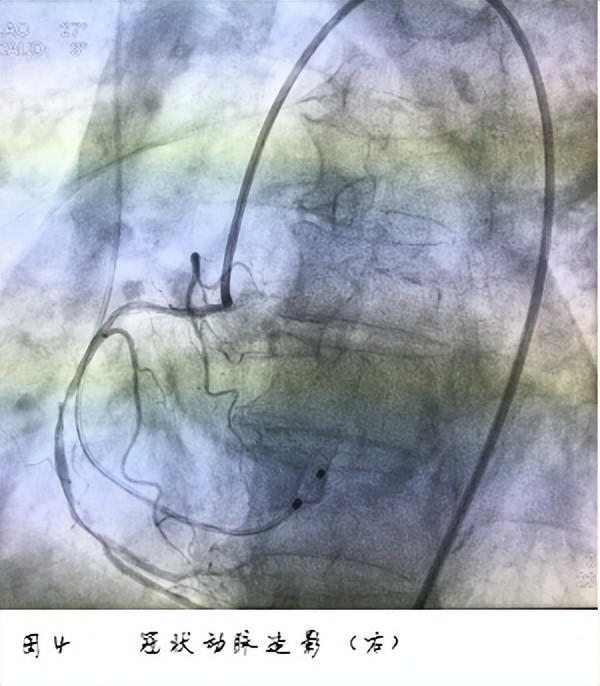
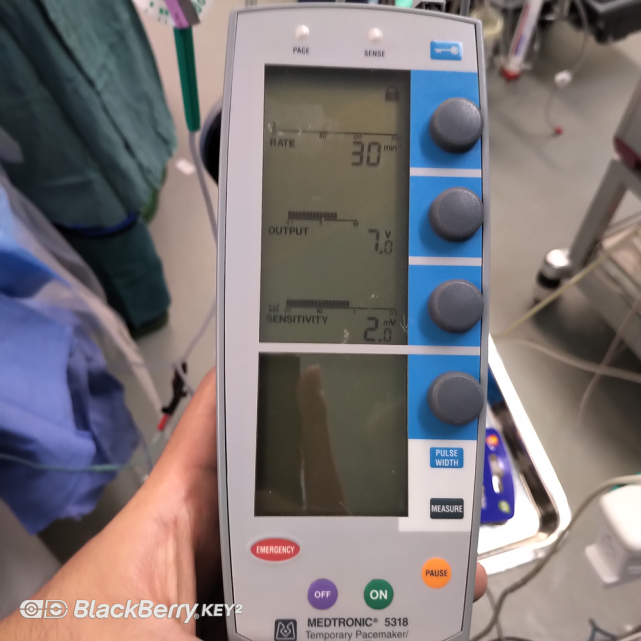
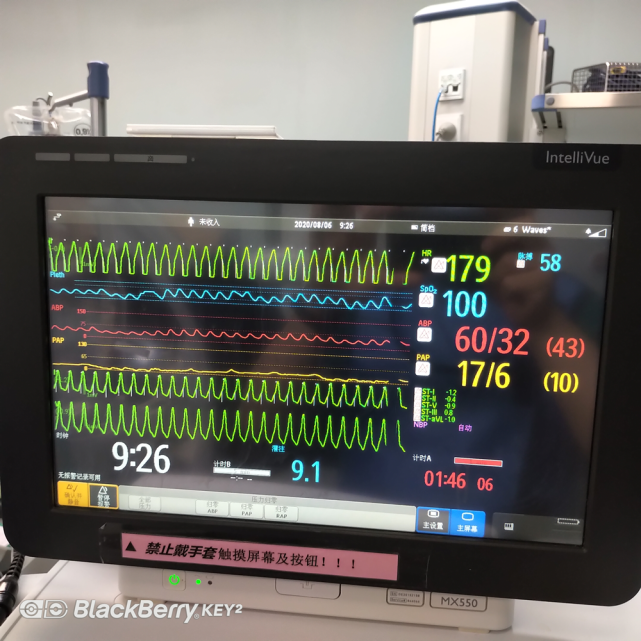
6) At the beginning of the surgery, after heparin, ACT> 300 seconds, after hepatinization meets the standard, the anesthesiologist needs to understand the coronary condition of the patient and clarify whether the patient needs to solve the related problems of the coronary vein in one stop. The surgeon is a temporary pacemaker for the patient to confirm the location of the temporary pacemaker, the pace perception effect and the pacemaker parameter setting. 7) During the surgery, when the surgeon performs an expansion of the valve, placed the valve, and the expansion is expanded, the patient needs to be treated with "speeding". After stopping, the patient's ECG monitoring is needed. Whether the ECG has autonomous arrhythmias, whether it is merged and quickly causes death, derived arrhythmia, bundle trimming or conduction block. If severe arrhythmia occurs, it should be corrected in time.
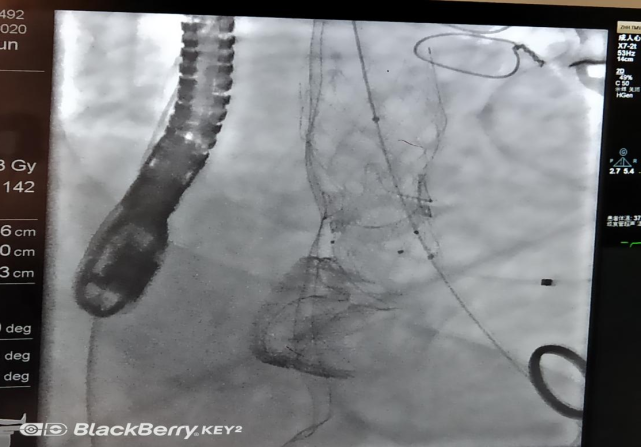
8) After surgery, the surgeon will evaluate the patient's immediately surgery effect after surgery based on the film image and ultrasound. The surgical effect is satisfactory to prepare for anesthesia and prepare to attract the secretions of the patient's trachea and oral cavity. Strictly monitor the patient's life signs, observe the patient's anesthesia awakening status, and meet the evaluation standards that can be removed by the tracheal intubation. After removal, the general status and life signs of the patient should be tightly monitored. Essence
9) Patients have good observation of general conditions and stable vital signs, which can be transferred back to the guardian to continue treatment.
I believe that with the advancement of science and technology, the continuous accumulation of surgical experience, the continuous efforts of staff in all aspects of the team will benefit a large number of patients because of our work, improve the condition of the disease, and improve life treatment.
Author: Wang Jianyue, a post -80s of the indigenous area in Beijing, came from the background of a medical family. He studied at China Union Medical University and now works at the Anesthesia Center of Beijing Anzhen Hospital.

[Reminder] Pay attention, there are a large number of professional medical sciences here to reveal those things about surgical anesthesia ~
- END -
Do you want to puncture the lung nodule?Teach you to judge you

*For medical professionals for reading referenceSolution clinical confusionWith mo...
"Sit" in front of the old man's table to "sit" out of the pulmonary embolism, doctor: avoid sedentary and long stand, the weather is hot and hydrating

Wuhan Evening News July 27th News The front of the table was a whole day. Recently...