Which of the best blood pressure control target is the best?British experts question
Author:Cardiovascular Channel in the Time:2022.08.31
*For medical professionals for reading reference

ESC expert praise Chinese guide standards reasonable
There are still many patients in countries and regions, including China and regions that have not been able to control the standards. While doctors and patients need to work together, how can high blood pressure control be regarded as "reaching standards" in recent years, especially "strengthening the pressure". After proposing 130/80mmHg, which standard is more reasonable, it is worthy of debate.
At this year's European Heart Society (ESC) Annual Conference, the control of blood pressure focuses on the rationality and feasibility of blood pressure targets.
Anti -pressure can not ignore safety
Professor Bryan Williams from the University of London University of London, the University of London, introduced his main point of view: the reduction target cannot ignore security.
Professor Williams shared a common scene. Many other departments who do not understand the situation sometimes proposed: "Why not control the patient's blood pressure to the normal physiological blood pressure range?"
His answer was: "Because our patients have no normal physiological conditions ..."
Professor Williams believes that the blood pressure is reduced to a certain degree. The benefits obtained by the antihypertensive therapy and the damage to the patient have reached the point where it needs to be measured and discussed (as shown below). Today, some radical new standards may cause the damage of antihypertensive than the benefits of lowering blood pressure.
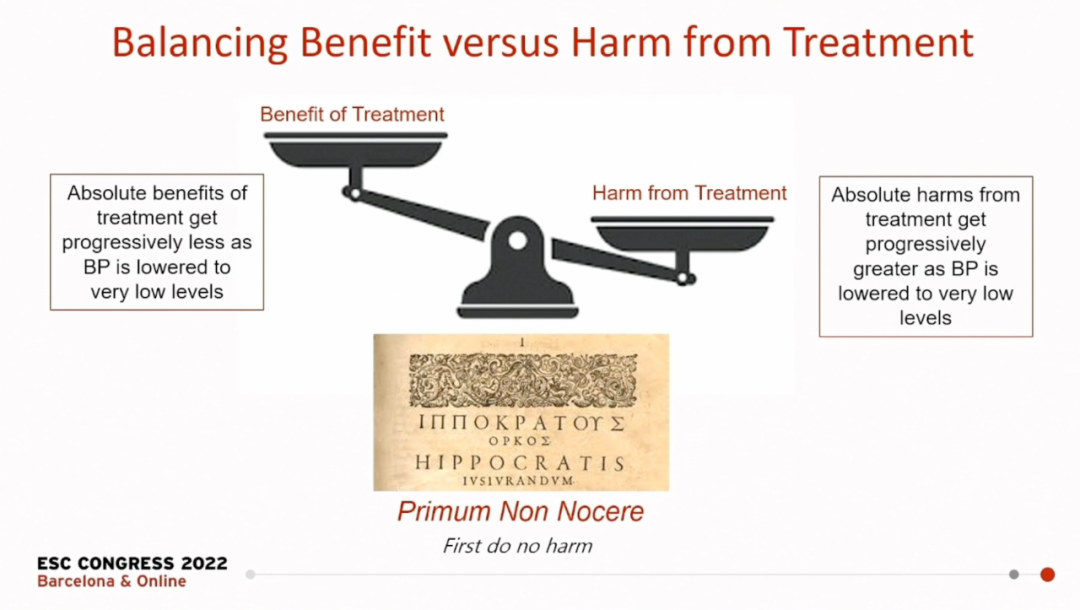
figure 1
He believes that the following basic considerations should be made to formulate a reduction target:
1. Evidence. The goal of treating antihypertensive should be that there is sufficient evidence to prove that the risk of cardiovascular disease can be reduced, and the safety and patient tolerance are guaranteed;
2. Individualization. The "best" blood pressure target is not the best choice for each patient. Consider the age of the patient, complication, tolerance, blood pressure baseline, etc.;
3. Safety. The goal of the guide should be "safe to everyone", so the guide policy is also conservative.
Guidance goals are chaotic, many clinical debates
Professor Williams pointed out that the current guidelines in different regions of the world have begun to become politics, and have their own views on the antihypertensive target.
Table 1
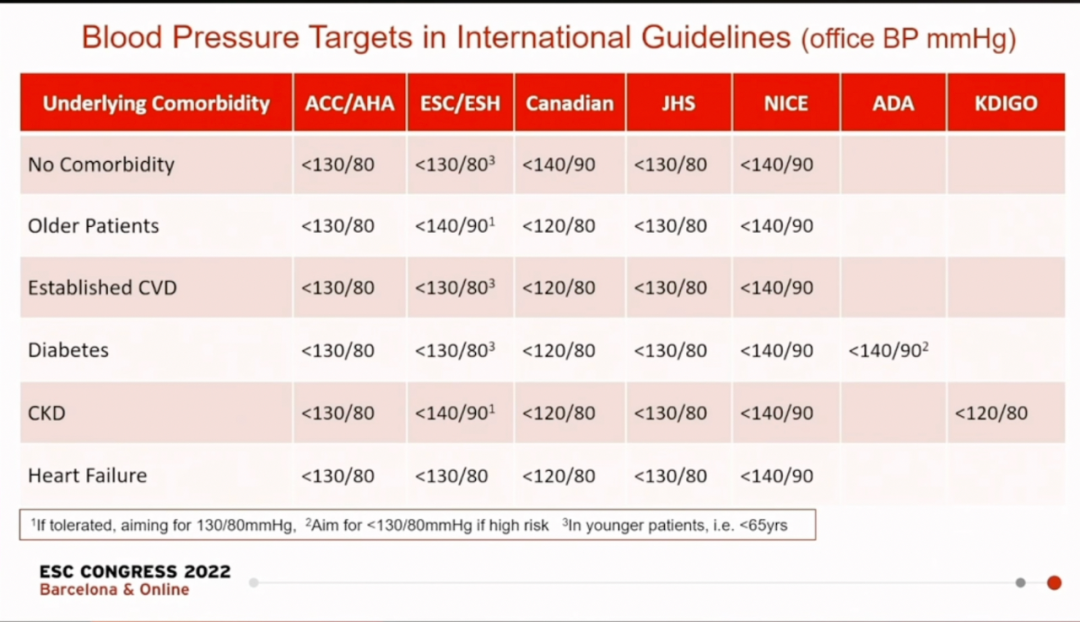
It can be seen that the American Cardiac Society (ACC)/American Heart Association (AHA) and Japan Hypertension Management Guide (JSH) Guide to patient病 Patients with chronic kidney disease (CKD) and patients with heart failure have formulated 130/80mmHg blood pressure control targets, while the British National Health and Clinical Optimization Research Institute (NICE) is unified at 140/90mmHg. The European Hypertension Society (ESH) has a choice to formulate elderly patients and CKD patients with an antihypertensive target of 140/90mmHg, and the rest is 130/80mmHg. At the same time, Canadian guidelines put forward more aggressive 120/80mmHg goals.
Professor Williams pointed out that there are many influencing factors that the guidelines choose blood pressure control targets, such as evidence of epidemiology and the mutual trade -offs and tug -of -tug of evidence of epidemiology and the evidence of random control. In the study of blood pressure control, the admission patients have the age of age and the baseline of the disease, so that the evidence cannot cover everyone.
In addition, in recent years, the champion analysis of random control research has played an important role in the formulation of the guide standards, but these gathered analysis hindered the subtle differences in individual experiments.
He introduced that the ESC guidelines are still targeted at the target of the systolic blood pressure below 140mmHg. If the patient can tolerate it, it is aimed at 130mmHg, but generally does not use 120mmHg as the goal and does not adopt the standard for strengthening the pressure.
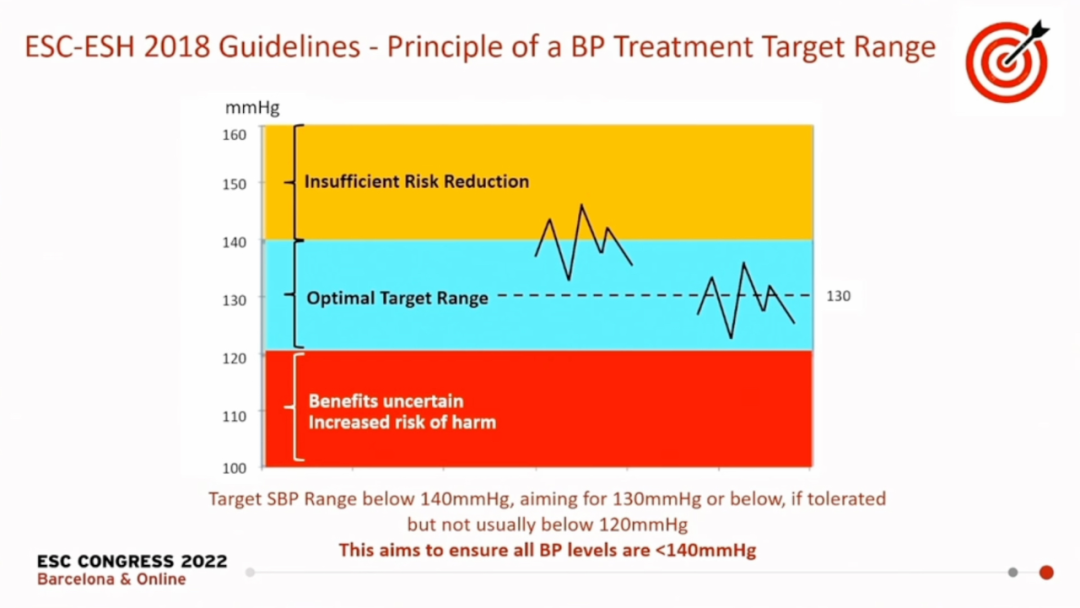
figure 2
The important thing is not the absolute value of the blood pressure,
Instead of maintaining blood pressure within the target range
Professor Williams believes that the effect of controlling blood pressure is more correlated with the time of blood pressure controlled within the target range. If the radical blood pressure control target only obtains a better blood pressure measurement value, the effect is poor.
As shown in the figure below, in the study of 140/90mmHg as a lower -voltage target, we focus on controlling the patient's blood pressure for a longer period of time within this range, and the health advantage obtained is even greater than strengthening the pressure.
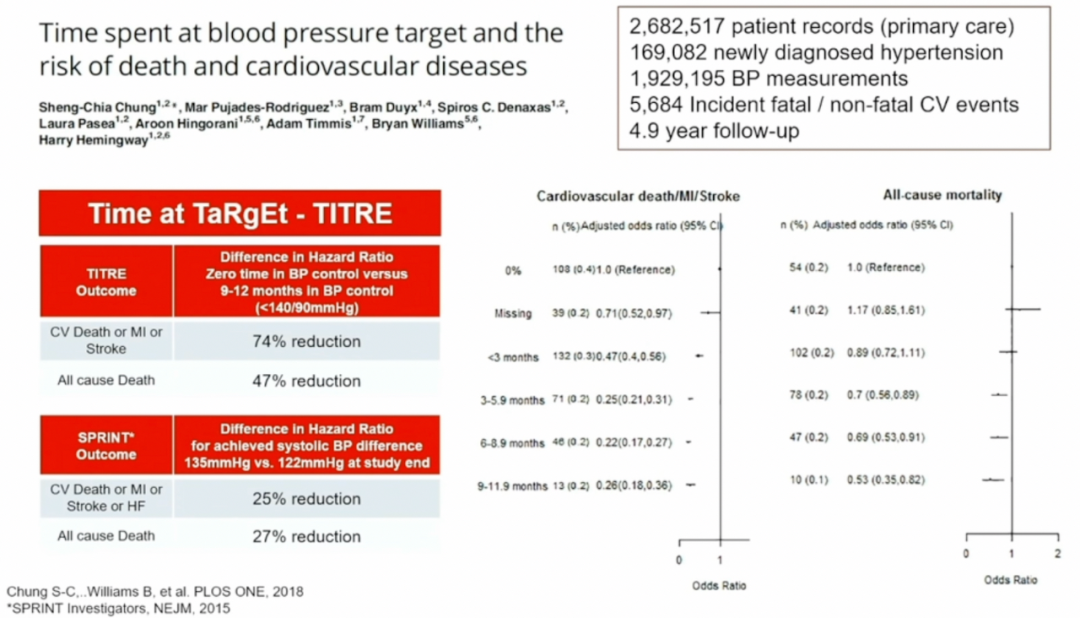
image 3
Overall, Professor Williams supports ESC's own guidelines, and does not recognize the strengthening of the antihypertensive standard. And he believes that when choosing blood pressure standards, clinicians 'considerations of patients should be more inclined to observe the age of biological age instead of stereotypes, that is, considering patients' complications, weak physical condition, and whether they can withstand more radical antihypertensive treatment It is still necessary to choose a more secure and safe solution.
New standards for China Standards Join Discussion
Professor Cai Jun, Fuwai Hospital of the Chinese Academy of Medical Sciences, introduced the practical experience of China's high blood pressure control at this ESC annual meeting.
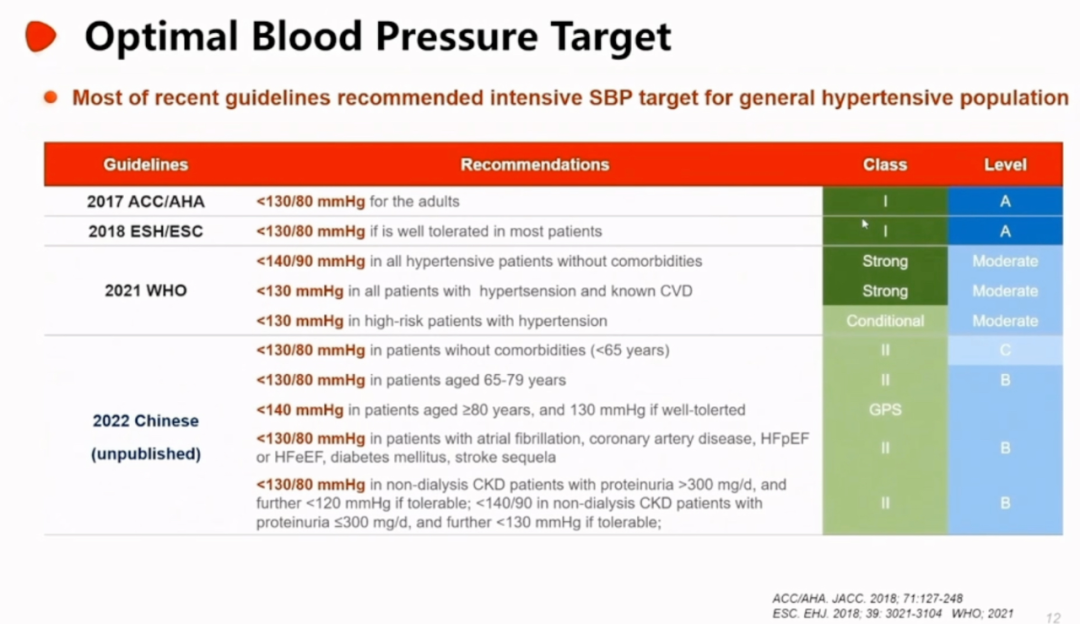
Figure 4
Professor Cai introduced that the high blood pressure control goals recommended by the China Guide in 2022 are as follows:
1. Patients with an age of 65 years old, the target of blood pressure control is <130/80mmHg;
Patients between 2.65-79 years old, the target of blood pressure control is <130/80mmHg;
3. Patients who are not less than 80 years old, the target of the blood pressure control is <140mmHg. If the tolerance is better, it can be recommended <130mmHg as the target; 4. Atrial fibrillation, coronary arteries, ejection scores (EF) retained heart failure retained (HFPEF) or patients with normal heart failure (HFEEF), diabetes, sequelae of diabetes, sequelae of diabetes, and sequelae of stroke, the target of blood pressure control is <130/80mmHg;
5. Patients with non -dialysis CKD, urine protein> 300mg/d, and the recommended blood pressure target is <130/80mmHg. If you are tolerated, you can recommend <120mmHg; non -dialysis CKD patients, urine protein ≤ 300mg/d, recommended blood pressure control target target For <140/90mmHg, if you are tolerated, you can recommend <130mmHg.
Professor Cai also introduced China's experience and standards for lifestyle intervention and drug control blood pressure, and outlook for more research directions in the future.
Interview after the meeting, Professor Williams Professor Ren Ren's guidelines
(Professor Bryan Williams answered "Medical Community" questions)

ask
Why are the guidelines formulated differently based on the same evidence? Is the differences in factors such as race affected this problem? For example, white and East Asians may be suitable for different antihypertensive targets?
Answer: The reason why the US standards are different from the European standards is that the standard of 130/80mmHg set by the United States is to include the use of lifestyle improvement, and European standards are similar to China. 140/90mmHg is based on the need to use drug control. The standards are set, and I think the latter is more reasonable.
It is not appropriate to set the standard of 130/80mmHg for the patient's baseline of the patient's body. The European standard believes that if you can tolerate 130mmHg, then consider this situation, but the US guide recommends that everyone should reach 130/80mmHg the following. In fact, the entry objects of Sprint's research have been screened. They are patients with low blood pressure and are not very high. The baseline data is also good, so they can achieve 130/80mmHg.
However, we clinically encountered patients with 180mmHg systolic blood pressure, and the drop to 130mmHg means that the pressure is reduced by 50mmHg at once. Considering the tolerance and safety, the patient's own baseline. Not suitable.
The 120MMHG standards proposed by Canada are even more unrealistic. It is a wonderful dream, and I don't think they have evidence to support them.
As for whether the difference between human race causes different blood voltage targets, after listening to the Chinese guidelines just now, it is very similar to the European standards, and the idea of Chinese guidelines is also very coherent. "First of all The selected standard, if you can tolerate, choose a lower voltage reduction target ", similar to European guidelines. Therefore, I want to say that the one here should agree that the difference between human race has no effect, and we can use similar antihypertensive targets.
Where can I look at the latest reports of cardiovascular?
Source of this article: Cardiovascular Channel in the medical community

Author of this article: Jiang Feixiong
Editor in charge: Peng Jianping Peng Sanmei
- END -
Epidemic tips: Hand -hygiene is really important!Did you wash it right?
The Yangtze River Daily Da Wuhan Client August 27th News New Crown Pneumonia's epidemic prevention and control and hand hygiene is really important! Hubei Disease Control reminder: We must continue t...
Henan yesterday added 9 new natives of infection
At 0-24 on August 18, there were 9 cases of new local infections in the province (4 cases of 4 cases of Suiping County, Zhumadian City, 4 cases of Fo County, Anyang City, and 1 case of Chuanhui Distri